In late December of 2024, I mourned myself, perhaps prematurely.
It came almost exactly on the 20th anniversary of my first 5K, which is probably why I’m still here to discuss it.
I’ve known since 2010 that I had a very high CAC score, but 15 years ago my exercise stress test was normal, so it was mostly just a warning to stay active, keep eating healthy and take my meds.
That changed in 2024, when my new PCP was worried by that long-ago CAC, and recommended some follow-up testing.
Because I felt great during my 10x Ironman near the end of 2024, with absolutely no symptoms of any kind, it was a real gut punch when a month of tests including an exercise stress test, nuclear myocardial perfusion imaging, and a coronary CAT scan (CCTA) revealed I had moved beyond simply having a boatload of risk to having active cardiovascular disease that required action.
My January 2025 CCTA flagged likely significant blockages in the left anterior descending artery (the LAD, or widowmaker) and a chronic total occlusion, or “CTO” – a fully blocked obtuse marginal artery (OM2), which is a branch of the circumflex. Another very small artery, the ramus, was fully blocked.
Fortunately, testing also identified helpful collateral circulation, where newer vessels had grown to provide blood flow the OM2 CTO could not. Of course, that raises a big question: how much blood flow was my heart actually getting through the “mini spare” – those collateral vessels.
We got at least a partial answer from my exercise stress test. Severe inducible ischemia was present during exercise, but absent at rest. That meant the collateral circulation supplied enough blood at rest to keep things working, but it couldn’t completely make up for the lost blood flow related to that CTO of the OM2 vessel.
In fact, that collateral flow to the area of the heart normally supplied by the OM2 was the main reason I hadn’t had a heart attack.
Plus, that early report also assessed that I had a normal ejection fraction and practically normal fractional flow reserve (FFR). This was somewhat encouraging, since it seemed to conflict with the report of severe blockage.
“Nobody here gets out alive.”
The Doors musical frontman Jim Morrison once famously said, “No one here gets out alive.”
It’s a simple truth about impermanence, but every time I hear it, it sounds like a hostage threat.
That’s how I felt when I got the news from the stress test and the CCTA.
I suddenly felt, and continue to feel, very mortal.
Now I’m entering a new chapter in my life: fresh uncertainties, compromises, and difficult judgment calls.
What’s my blood pressure right now? My BG’s dropping, will it cause an arrhythmia? How does my chest feel? What’s my emergency plan if I have a massive heart attack out on a run? Is it safe to ride when it’s hot? What if something happens when I’m swimming at the lake? Did I bring the unbuffered full-strength aspirin? Do I have the nitro in my pocket? Can Leslie locate my phone to tell 911 where to pick me up? Will I survive it? Will I even FEEL it if I have a heart attack?
This is not the post I wanted to write on my 20th anniversary of embracing physical activity and confronting my hypoglycemia fears.
This can’t be that post, I keep telling myself.
But this IS that post.
I find myself looking back on the last two decades as if it were a dream, as if it happened to someone else, and as if the unsettling reality I’m now in is one where I never laced up my running shoes at all.
But off and on, I keep encountering people in similar situations, like the folks in the Cardiac Athletes Facebook group.
Fortunately for me, the group’s membership is mostly a bunch of super-badass ultra athletes who are still active despite heart attacks, arrhythmias, heart valve problems, stents, off-pump bypasses, minimally invasive bypass (MIDCAB), conventional bypass surgery and many other serious heart issues.
Some had procedures before a major cardiac event, some only after obvious symptoms or something imminently life threatening, like a heart attack. Some had single-vessel coronary artery disease; some had totally asymptomatic coronary artery disease. Just like me.
Then I don’t feel so alone. Even though I haven’t met anyone in the group who has Type 1.
Going deeper
Given some of the inconsistencies I mentioned earlier, I needed more definitive answers.
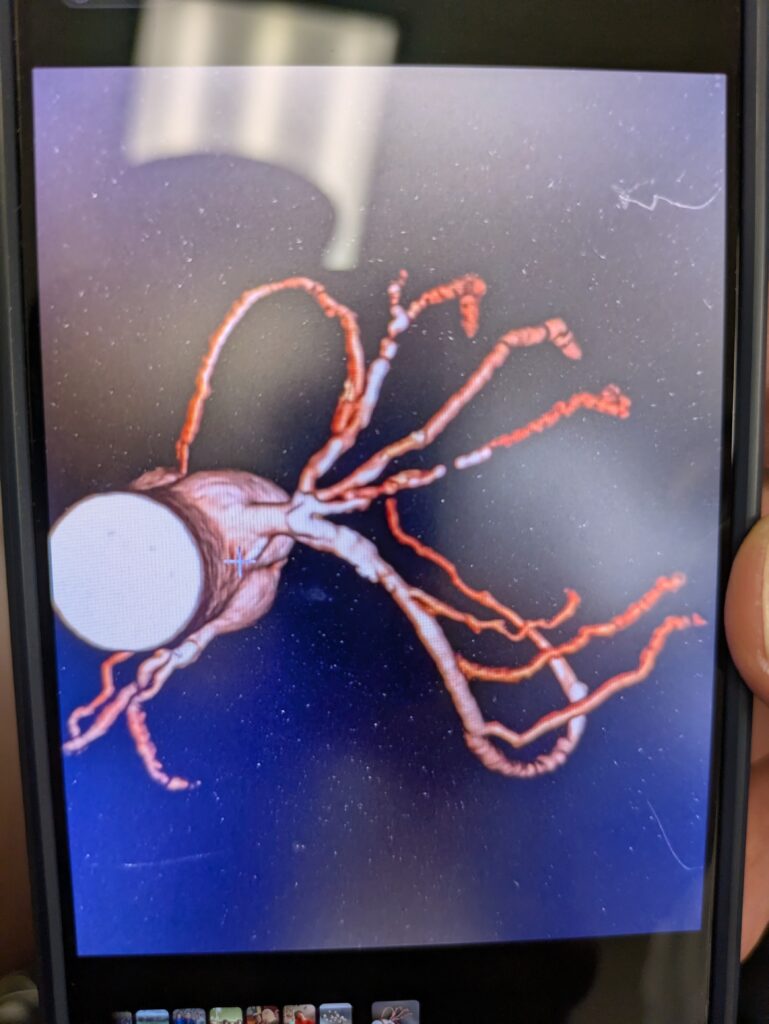
So on March 19, 2025, I underwent cardiac catheterization. This is an invasive procedure where a cardiologist inserts a tiny tube into a blood vessel and guides it all the way up to the heart. Then, they release tiny bits of dye to help identify blockages and other issues while imaging tools take pictures of areas the dye can–and can’t–reach.
I arrived at my local hospital just before 6 AM. Prep for the procedure took an hour or two. They explained the process, put in an IV and took a blood sample, and wheeled me up to the cath lab. Another nurse prepped the site in my groin where the introducer needle would go for the cath wire the interventional cardiologist would use to fully investigate the previously reported blockages.
It was a full-day affair, and I finally left the hospital in the late afternoon, this time shocked for a different reason.
The news was better than expected.
The catheterization confirmed that the OM2 artery indeed was fully blocked. However, it also found that the LAD was calcified but had only “mild” atherosclerosis. This means that although I have a lot of calcified plaque in the walls of my LAD artery, which is definitely not good, it also hasn’t dramatically reduced the blood flow through that vessel yet.
So I’ve gone from expecting immediate stenting or bypass surgery to address multivessel blockages to something more like watch-and-wait.
But wait for what? And watch how often? And since I have no angina or other symptoms thanks to T1D cardiac neuropathy – would my first symptom be something like a heart attack or sudden cardiac arrest?
Ironically, it’s all now much more complicated.
If I had symptoms or extensive non-total blockage, stenting or bypass would be the immediate answer.
But without symptoms – even though I’m in a very high risk cohort and asymptomatic precisely because of the very disease that places me in that cohort – no one’s quite sure what’s best.
For the moment, I’m staying active while keeping my heart rate below the ischemic threshold, checking for early arrhythmias with a Kardiamobile, and working to figure out a longer-term plan.
May 2025 UPDATE: I’ve met with a cardiologist with expertise specifically in CTOs who has a plan for reassessing my ischemia, and has also referred me to a sports cardiologist. Stay tuned.
Dodging a bullet <> bulletproof
Despite the better-than-expected news, I still feel quite mortal. There’s no going back after this.
When you come to the heart disease party with 50+ years of Type 1 under your belt, you have to manage everything to get as many good years as possible. You don’t get a bye on anything.
A1C. Blood pressure. Heart rate. LDL. Apo(b). Apo(a). All the meds. Sleep.
Figuring out how to reap the T1D benefits of exercise without causing a cardiac event.
But I apparently have a little more time to figure out what to do.
And during that time, I can do something useful and purposeful, even if it doesn’t change the outcome.
Like a Buddhist sand mandala, made by carefully pouring grains of sand into an intricate pattern that the artist knows won’t last.
A lesson my dad taught me…five years after he died
All of this reminds me how lucky and privileged I’ve been to get this far.
I’ve had time to run tests, consult experts, and get a diagnostic cardiac cath done before it was an emergency.
It gives me hope. But like the sand mandala, it reminds me that our time here is not permanent.
If we want to do or say something important, now’s the time.
A few months before my dad died in 2020, he made it a point to to tell family and friends how he felt about them. I knew he felt the cold wind at the door, and I reassured him that I was proud of him, that he’d been a great father. I knew that was my chance to tell him, while he could hear it and know it.
One of the lessons he still managed to teach me–five years after his passing (my God, has it really been that long?)–is that we all need to say the quiet parts out loud, while we can.
So whatever happens, that’s the lesson I want to learn from it: that the only moment we have is now, and that’s when to say and do the things that matter.
Once you recognize the transience of all things, life is oddly easier.
Grudges don’t hold. Arguments don’t last. You think twice about whether a sharp comeback during an argument is truly the last thing you’d want your loved one to hear.
I had a similar epiphany in 1988 when I survived an armed robbery. I was so glad the last thing I had said to Leslie was that I loved her and would see her soon.
It really doesn’t matter if you’re cut off in traffic. It doesn’t matter if someone said something hateful–it’s probably just a reflection of their pain anyway. It doesn’t matter anymore who’s right or who’s wrong. None of that matters, and clinging to it does more harm than good.
Instead, I plan to take more time to watch the sunrise and appreciate the flickering beauty that is life.